Ureteroscopy (rigid and flexible)
Investigation and removal of urinary calculi by the natural route
What is ureteroscopy (rigid or flexible)?
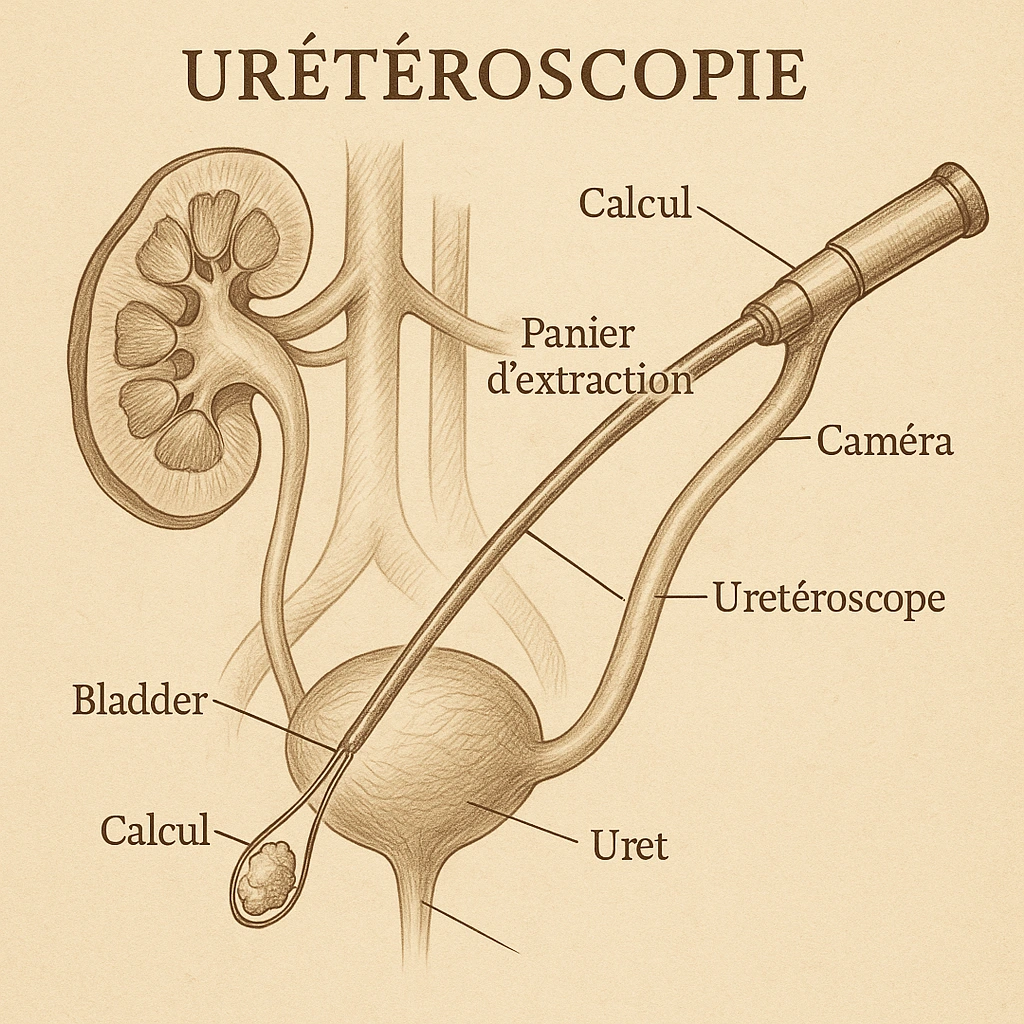
Ureteroscopy is an endoscopic urological procedure that allows access to the upper urinary tract (ureter, renal pelvis, caliceal cavities) via the natural tract – without surgical incision. There are two types:
- Rigid ureteroscopy: mainly used for calculi located in the ureter (pelvic segment, iliac segment, etc.), or to extract fragments, insert probes, etc.
- Flexible ureteroscopy: allows navigation through the kidney cavities, including the calyces, thanks to a flexible, thinner and more malleable endoscope, adapted to anatomical curvatures.
📌 The main objective is direct exploration of the excretory system, visualization of the calculus and then its fragmentation (usually by laser) or extraction (forceps, basket) via these natural routes, without opening the skin.

When is this procedure recommended?
Main indications
Rigid or flexible ureteroscopy is indicated in the following situations:
- Urinary calculi resistant or inaccessible to extracorporeal lithotripsy (ECL), particularly dense (> ~ 1,000 Hounsfield units) or hard (e.g. cystine calculi).
- Moderate-sized calculi (< ~ 20 mm) in the ureter or kidney, when LEC is not effective or possible.
- Renal localization, particularly in the lower calyces or in malformed kidneys, or when the kidney is difficult to access for lithotripsy.
- Alternative to LEC if contraindicated (e.g. patient on anticoagulant therapy, unfavorable anatomy, high stone density).
Limitations and contraindications
- Untreated urinary tract infection.
- Difficult ureteral anatomy (stenosis, history of ureteral surgery, path anomalies, very large prostate) that prevents access or passage of the device.
- Very large stones (> ~ 20-25 mm), or coralliform or very complex stones, for which other techniques (percutaneous nephrolithotomy) are preferable.
How does the procedure work?
Here are the typical steps involved in flexible or rigid ureteroscopy, for the exploration and removal of urinary calculi:
Preparation
- Imaging (injection-free CT scan, ultrasound, possibly X-ray) to locate the stone precisely, measure its size and assess its density.
- ECBU (urine cytobacteriological examination) to check sterility or treat an infection prior to surgery
- Anaesthesia: often general for flexibility, sometimes local or spinal depending on the patient’s condition and the location of the stone.
- Sometimes a double-J catheter is inserted to dilate the ureter (“prepare” the passage for the ureteroscope), if necessary.
Intervention
- Introduction of the urethroscope through the urethra, then the bladder, then into the ureter; for the flexible version, progression to the renal cavities if required.
- Visualization of the calculus, fragmentation (Holmium YAG laser most often) if too large to be extracted directly.
- Extraction of fragments or whole calculus with forceps or endoscopic basket.
- At the end of the operation, a double-J catheter (ureteral endoprosthesis) is usually inserted to drain the ureter, prevent edema, facilitate evacuation of fragments or provide relief.
Post-operative care
- Short hospital stay, often on an outpatient or 24-hour basis depending on the case.
- Moderate pain, possible transient urinary bleeding, occasional discomfort associated with the double-J catheter (tugging, frequent urges).
- Analgesics, possibly anti-inflammatories prescribed.
- Control of renal function, urine monitoring.
- Removal of double-J probe according to protocol (a few days to a week depending on tolerance and site of calculus).
- X-ray or imaging check a few weeks later, to ensure that no residual lithiasis fragments remain.
⚠️ Expected results
- A high success rate for pelvic ureter stones, often > 90%.
- For moderate-sized kidney stones (< ~1 cm), good results; for sizes between 1-2 cm, less success, and sometimes the need for several operations or additional treatment.
⚠️ Possible complications
- Transient hematuria (bleeding in the urine) after the procedure.
- Pain or discomfort (colic, clot, ureteral spasm) in the days that follow.
- Urinary tract infection, even more severe if sampling or fragmentation with untreated pre-existing infection.
- Risk of ureteral injury (perforation, laser burn, avulsion, or trauma) to be handled with care.
- Remote ureteral stenosis in some cases.
Why choose this technique rather than an incision or other method?
✔ Minimally-invasive: no open surgery, no scarring, less trauma, faster recovery.
✔ Natural route management: access is via the urethra/bladder, avoiding any external incisions.
✔ Reaches stones that could not be expelled spontaneously or treated effectively by other methods (LEC in particular).
✔ Good compromise between efficacy, safety and comfort for many patients.
Pre- and post-operative
Pre-op: what you need to know
- The patient will need to undergo a number of tests prior to surgery: imaging (non-injected CT scan, ultrasound) to locate the stone and measure its density and size.
- Check for urinary tract infection (ECBU), and treat if necessary.
- Information on anesthesia and hospitalization (outpatient or 1-day, depending on the facility).
- Check current treatments (anticoagulants, antiaggregants), possible adjustments.
- Discussion on the possible insertion of a preliminary probe (double-J) if the ureter is not dilated enough for the endoscope to pass.
After the operation: follow-up
- Moderate pain expected, slight bleeding possible, often for a few days.
- Painkillers / anti-inflammatories as required.
- Drink plenty of fluids to help eliminate lithiasis fragments.
- In the event of a double-J probe, it will be removed according to protocol (a few days to a week or more depending on the situation).
- A radiological/imaging check a few weeks later to ensure that no fragments remain.
- Urological follow-up to monitor complications such as stenosis, infection and catheter-related discomfort.
Ureteroscopy specialist
Dr. Dominique will determine whether ureteroscopy is the best option for your case, compared to other methods such as lithotripsy, percutaneous nephrolithotomy, etc.
✔ He will assess the risks associated with your general condition, the size, location, composition of the stone, and your urinary anatomy.
✔ It also ensures follow-up, evacuation, post-operative monitoring, and adapts treatment according to results.
My video review
I’ve made this video to explain flexible and rigid ureteroscopy in detail.
Make an appointment
Dr Sébastien Dominique offers you a personalized assessment, an adapted procedure, and attentive follow-up to guarantee the best possible result.